Neuroradiology
Facet Joint Block / Injection
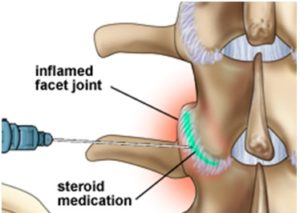
A facet joint block is an injection of local anaesthetic into one or more of the facet joints. These joints are found in the spine where they connect the vertebrae to each other. They allow the spine to bend and twist. Like a knee or hip, facet joints have cartilage between the bones and a fluid-filled capsule to allow for smooth movement. When damaged, facet joints can cause debilitating pain in the neck or back.
Multiple injections may be performed, depending upon how many joints are involved. Facet joint blocks are typically requested for patients who have pain primarily as a result of arthritic changes in the facet joints or for patients who have mechanical pain. A facet joint block may be diagnostic (a test to see if your pain is coming from this area), and/or therapeutic (to relieve your pain).
When is a Facet Joint Injection Done?
A facet joint injection is performed to treat neck and back pain in combination with other non-surgical spine treatments like rest, medications and physio therapy.
These injections are used to treat pain and to identify the painful joint(s). If an injection successfully treats the pain, it will confirm that a particular facet joint is causing the problematic pain
How is a Facet Joint injection Done?
In order to guide the injection to the facet joint, your pain specialist will use fluoroscopic (X-ray) guidance during the injection. This will allow the physician to see the joint and ensure that the needle is in place before injecting the anesthetic-cortisone mixture. The procedure takes between 5-15 minutes. Thanks to the anesthetic used, the injection can provide immediate pain relief.
Vertebroplasty
Relieves Spinal Compression Fracture Pain, Strengthening Weakened Vertebrae
A surgical filling of the vertebrae which restores original shape and configuration, relieving pain caused by spinal compression.
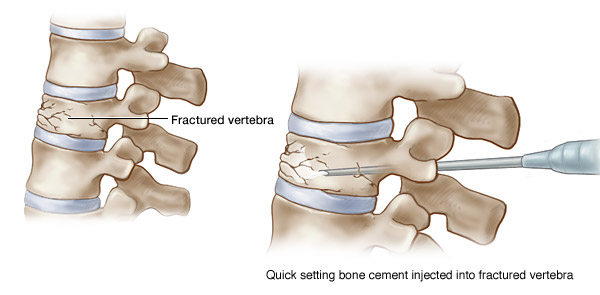
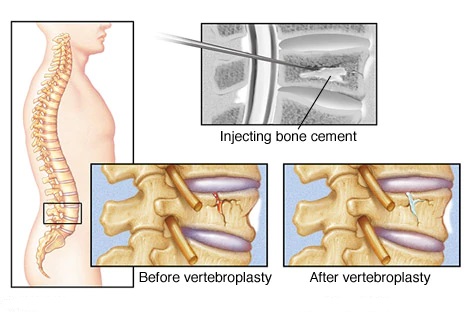
Vertebroplasty and kyphoplasty are procedures used to treat painful vertebral compression fractures in the spinal column, which are a common result of osteoporosis. Guided by fluoroscopy (x-ray), the physician inserts a needle into the damaged vertebra and injects specially formulated bone cement into the fractured bone (vertebroplasty) or insert a balloon into the fractured bone to create a space and then fill it with cement (kyphoplasty). Following vertebroplasty, about 75 percent of patients regain lost mobility and become more active.
How Long does the Procedure Take?
Vertebroplasty is safely performed on an outpatient basis. The procedure takes about one hour. Afterwards, there is a short period of observed recovery time.
What are the Expected Results?
Vertebroplasty has been delivering excellent outcomes since the early 1990s, achieving dramatic results in up to 90 percent of cases. Some patients experience immediate pain relief and most report that their pain is gone or significantly better within 48 hours. Typically, patients resume normal activity within 24 hours. Vertebroplasty resolves pain, stabilizes fractures, increases functional abilities, and reduces spinal deformity without surgery or prolonged recovery. By repairing the fracture, vertebroplasty promotes lasting pain relief.
How does the procedure work?
When a vertebra breaks or fractures, bone fragments develop. Pain occurs when these fragments slide or rub against each other or protrude into the spinal cord.
Vertebroplasty involves injecting the bone with a cement mixture to fuse the fragments, strengthen the vertebra and provide pain relief.
First, the skin is numbed with a local anaesthetic. Then, using imaging guidance, the hollow needle or trocar is passed through the skin into the vertebral body for injection of the cement mixture into the vertebra.
In kyphoplasty, after numbing the skin locally, a balloon is inserted through the trocar into the fractured vertebra where it is inflated to create a cavity for cement injection. The balloon is removed prior to injecting cement into the cavity that was created by the balloon.
What are the benefits vs. risks?
Benefits
- Vertebroplasty and kyphoplasty can increase a patient’s functional abilities and allow return to the previous level of activity without any form of physical therapy or rehabilitation.
- These procedures are usually successful at alleviating the pain caused by a vertebral compression fracture; many patients feel significant relief almost immediately or within a few days. Many patients become symptom-free.
- Following vertebroplasty, about 75 percent of patients regain lost mobility and become more active, which helps combat osteoporosis. After the procedure, patients who had been immobile can get out of bed, and this can help reduce their risk of pneumonia. Increased activity builds more muscle strength, further encouraging mobility.
- Usually, vertebroplasty and kyphoplasty are safe and effective procedures.
- No surgical incision is necessary—only a small nick in the skin that does not need stitches.
Risks
- Any procedure where the skin is penetrated carries a risk of infection. The chance of infection requiring antibiotic treatment appears to be less than one in 1,000.
- A small amount of orthopedic cement can leak out of the vertebral body. This does not usually cause a serious problem, unless the leakage moves into a potentially dangerous location such as the spinal canal or the blood vessels of the lungs.
- Other possible complications include infection, bleeding, increased back pain and neurological symptoms such as numbness or tingling. Paralysis is extremely rare.
- Approximately 10 percent of patients may develop additional compression fractures after vertebroplasty or kyphoplasty. When this occurs, patients usually have relief from the procedure for a few days but develop recurrent pain soon thereafter.
- There is a low risk of allergic reaction to the medications.
- suitable for patients with spinal curvature such as scoliosis or kyphosis that results from causes other than osteoporosis.
- applicable for patients who suffer from spinal stenosis or herniated disk with nerve or spinal cord compression and loss of neurologic function.