Gynae / Urological Radiology
Uterine Fibroid Embolisation (UFE)
Fibroids are benign (non-cancerous) tumour’s, that arise from the muscular wall of the uterus. They are also known as leiomyomas and myomas. Fibroids are common and are detected in about 30% of women over the age of 30.
Symptoms:
These depend on the number and size and where the fibroids are. They may cause:
- Heavy menstrual bleeding that can cause anaemia
- Pelvic pain, pressure or heaviness in the abdomen, pain during intercourse.
- Bladder or bowel pressure which may result in the need to pass urine frequently or constipation.
- Infertility and problems during pregnancy
Treatment:
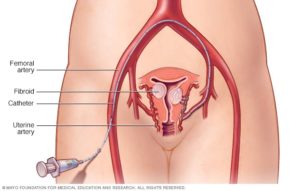
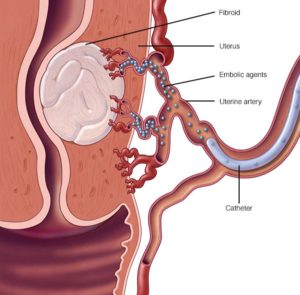
Most fibroids don’t cause symptoms and do not need treatment. For symptomatic fibroids there are medical surgical and embolisation treatment’s available. Uterine fibroid embolisation (UFE), is a procedure performed by a radiologist in a specialised x-ray suite. The physician uses x-ray imaging to guide small particles to the blood vessels supplying the fibroids. The small particles are injected through a thin flexible tube called a catheter. These particles are smaller than a grain of sand and are injected into the artery, blocking the blood vessels supplying the fibroids. It doesn’t matter how many fibroids are in the uterus because all of them are treated at the same time.
Pelvic pain or cramps shortly after the procedure and for eight to 12 hours afterward is the most common side effect. Pain for as long as three to five days after the procedure is not uncommon and may require appropriate pain medication.
You should be able to resume your normal activities within a week. Until then, minimal activity is recommended.
Without blood supply the fibroids die off and then shrink, on average by 40-50%, over a 3 to 6-month period. Most patients have a significant improvement in their symptoms, both for heavy bleeding (80—90%) and pelvic pressure (80-90%) after 4-6 weeks.
The effect of fibroid embolisation on fertility is not fully understood, so is typically offered to women who no longer wish to become pregnant or who want to avoid a hysterectomy, however many women have healthy pregnancies after having this procedure.
Ovarian Vein Embolisation
Ovarian vein embolisation is a minimally invasive treatment for pelvic congestion syndrome. This condition is a collection of symptoms (pelvic pain/heavy periods and or painful intercourse) from the presence of enlarged or varicose veins in the pelvis. The condition is the result of the venous valves at the top of the ovarian veins being improperly formed or becoming dysfunctional. This allows venous blood to travel the wrong way into the pelvis engorging the pelvis with blood in the premenstrual to menstrual phase or sometimes all the time. Pelvic pain is usually at its strongest premenstrually to menstrually and is often associated with painful intercourse (dysparuenia).
Embolisation helps relieve pain by using imaging guidance and a catheter to close off faulty veins so they can no longer enlarge with blood.
During this procedure, an interventional radiologist inserts a catheter up the femoral vein and into the faulty vein(s). Using x-ray imaging and a contrast material to visualize the blood vessel, the interventional radiologist advances a to the treatment site. A synthetic material or medication called an embolic agent, often Dacron filaments-bearing coils, are used that clot the blood and seal the faulty vein.
Most patients experience some side effects after embolisation. Pain is the most common and can be controlled by medication given by mouth or through your IV.
Most patients leave the hospital within 24 hours of the procedure, but those who have considerable pain may have to stay longer. You should be able to resume your normal activities within a week.

What are the limitations of Ovarian Vein Embolisation?
Successful embolization without injuring normal tissue requires that the catheter be placed in a precise position. This means that the catheter tip is situated so that embolic material can be deposited only in vessels serving the abnormal area. In a small percentage of cases, the procedure is not technically possible because the catheter cannot be positioned appropriately.
Varicocele Embolisation.
Varicoceles are varicose veins of the testicles and scrotum that can (but not always) cause pain, infertility and testicular atrophy (shrinkage of the testicles).
Approximately 10% of men have varicoceles. They are most common in men ages 15-35 years. Among infertile couples, nearly 30% of men have varicoceles.
Varicoceles are caused when the one-way valves in the scrotal veins, which allow blood to flow from the testicles and scrotum back to the heart, become dysfunctional or fail. This causes the blood to pool and the veins to enlarge to form a varicocele.
Varicocele embolisation is a highly effective, minimally invasive alternative to surgery, performed by an interventional radiologist in a specialised x-ray suite, in an outpatient setting.
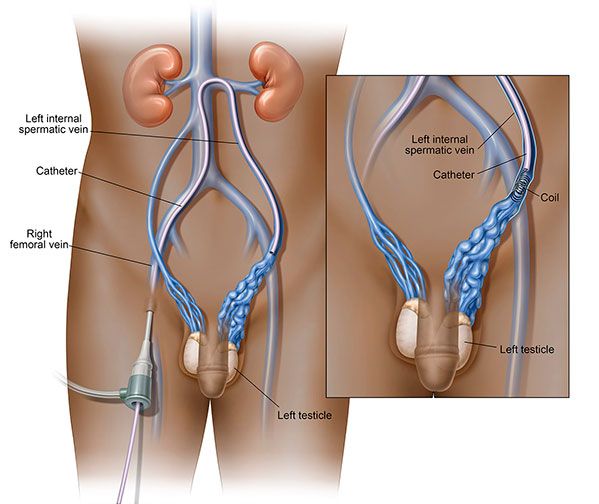
The doctor will insert a catheter through a small nick in the skin in your groin into your femoral vein. Using x-ray imaging and contrast media injections into the vein, they will feed the catheter into the affected testicular vein. The contrast injections help the doctor to clearly visualise the veins on the x-ray in order to pinpoint where the problem is and where to embolise, or block, the vein. Tiny coils made of stainless steel, platinum or other materials, such as liquids, which directly close a vessel, are then inserted in the vein to block blood flow to the varicocele. By blocking the diseased draining vein, abnormal blood flow into the testicle is stopped and the blood is diverted to healthy veins to exit the testicle through normal pathways. Swelling and pressure within the testicle will be reduced if the blood flow is successfully diverted.
When the procedure is complete, the catheter is removed and pressure is applied to stop any bleeding. Sometimes, your doctor may use a closure device to seal the small hole in the artery. This will allow you to move around more quickly. No stitches are visible on the skin. The tiny opening in the skin is covered with a dressing.
This procedure is usually completed within one hour.
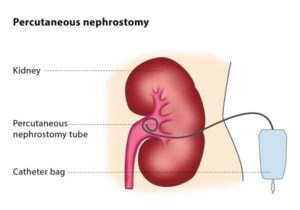
Nephrostomy Tube Insertion
Your kidneys are part of your urinary system and work to produce urine. Normally, the urine that is produced flows from the kidneys into a tube called a ureter. The ureter connects your kidneys to your bladder. When enough urine has collected in your bladder, you feel the need to urinate. Urine passes from the bladder, through your urethra, and out of your body.
A percutaneous nephrostomy tube is a catheter (plastic tube) that is inserted through your skin into your kidney. The nephrostomy tube is placed to drain urine from your body into a collecting bag outside your body when the ureter is blocked.
Sometimes there is a block in your urinary system and urine is unable to flow as normal. Blockages can be caused by several things, including: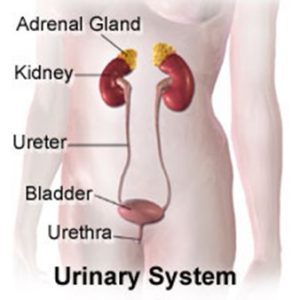
- kidney stones
- injury to the kidney or ureter
- an infection
- a congenital condition
- Tumour
Placing the Nephrostomy Tube
The procedure to place your nephrostomy tube typically takes less than an hour and will be performed under a local anaesthetic and sometimes sedation.
The doctor will inject local anaesthetic at the site where the nephrostomy tube is to be inserted. They will use Ultrasound and x-ray imaging to guide a very fine needle through the skin to the correct position. This position will be confirmed using and injection of contrast medium. Once the correct location is confirmed the nephrostomy tube system is positioned and fastened into position. The tube has a special “pig-tail” shape which helps keep it in position within the kidney. The tube is then fixed to the skin surface by a combination of sutures and special dressings. Once it is secured a drainage bag is connected to the nephrostomy tube to collect the urine that drains from the kidney.
When and if the nephrostomy tube drain is no longer required it is removed by medical or nursing staff. Often x-rays are used to guide the removal.
If you need the nephrostomy tube for a longer time, the tube will need to be exchanged periodically (usually every 3 months). This is a similar procedure, performed under local anaesthetic. The dressings and sutures will be removed and the pig-tail shape at the end of the tube will be released removed. A wire will be passed down the nephrostomy tube into the kidney. The old tube will be removed over this wire and a new tube will then be placed into the kidney over this wire. The tube will then again be secured the same as the old one.
Caring for your Nephrostomy Tube
The staff will instruct you on how to care for your nephrostomy tube. You’ll have to inspect your tube daily as well as empty any urine that has collected in the drainage bag.
Complications of a Nephrostomy Tube
Placing a nephrostomy tube is generally a safe procedure. The most common complication that you’re likely to encounter is infection. You should contact your doctor immediately if you experience the following symptoms, as they may indicate an infection:
- a fever over 38.3°C
- pain in your side or lower back
- swelling, redness, or tenderness at the site of your dressing
- chills
- urine that is very dark or cloudy, or smells bad
- urine that is pink or red
You should also contact your doctor should any of the following occur, as it may be a sign of a blockage:
- Urine drainage is poor or no urine has collected for over two hours.
- Urine leaks from the dressing site or from your tubing.
- The black mark on your tube (if there is a mark) has moved, or you see that your tube is longer than it was when it was put in.
- The nephrostomy tube comes out.
- There is blood, pus, or a bad smell coming from the place where the tube enters your skin.
Ureteral Stent Insertion.
Urine is normally carried from the kidneys to the bladder through long narrow tubes called ureters. These can become obstructed due to conditions such as kidney stones, tumours, infection or blood clots. When this happens physicians can use image guidance to place a thin flexible tube called a stent, in the ureter to restore the flow of urine to the bladder. One end of the tube is inside your kidney and the other end is in your bladder. Each end of the stent is shaped like a “pigtail”, this curl prevents movement of the stent.
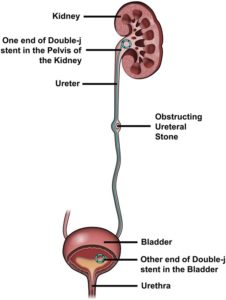 The procedure is very similar to a nephrostomy tube insertion. A needle / tube is passed via the skin into the pelvis of the kidney. The Doctor will then use x-ray imaging to attempt to feed a guidewire down the ureter, past the obstruction and into the bladder. Once this has been done the ureteric stent will be fed over the guidewire and into the ureter. It will be positioned so that one end is in the bladder and the other is in the pelvis of the kidney. A nephrostomy tube will also be inserted and clamped off. This is left in for a few days in case the stent does not drain the kidney adequately. The nephrostomy tube will be removed when the stent is deemed to be working well.
The procedure is very similar to a nephrostomy tube insertion. A needle / tube is passed via the skin into the pelvis of the kidney. The Doctor will then use x-ray imaging to attempt to feed a guidewire down the ureter, past the obstruction and into the bladder. Once this has been done the ureteric stent will be fed over the guidewire and into the ureter. It will be positioned so that one end is in the bladder and the other is in the pelvis of the kidney. A nephrostomy tube will also be inserted and clamped off. This is left in for a few days in case the stent does not drain the kidney adequately. The nephrostomy tube will be removed when the stent is deemed to be working well.
In the majority of patients, the stents are required for only a short duration, from a few weeks to a few months. However, a stent in the right position can stay in for up to three months without the need to replace it. When the underlying problem is not a kidney stone, the stent can stay even longer. It is up to your specialist to determine how long the stent remains in position for and they will discuss this with you.